Anatomy of the Lower Extremity Vascular System
The arterial anatomy relevant to the lower extremity circulation is demonstrated in Figure 1.
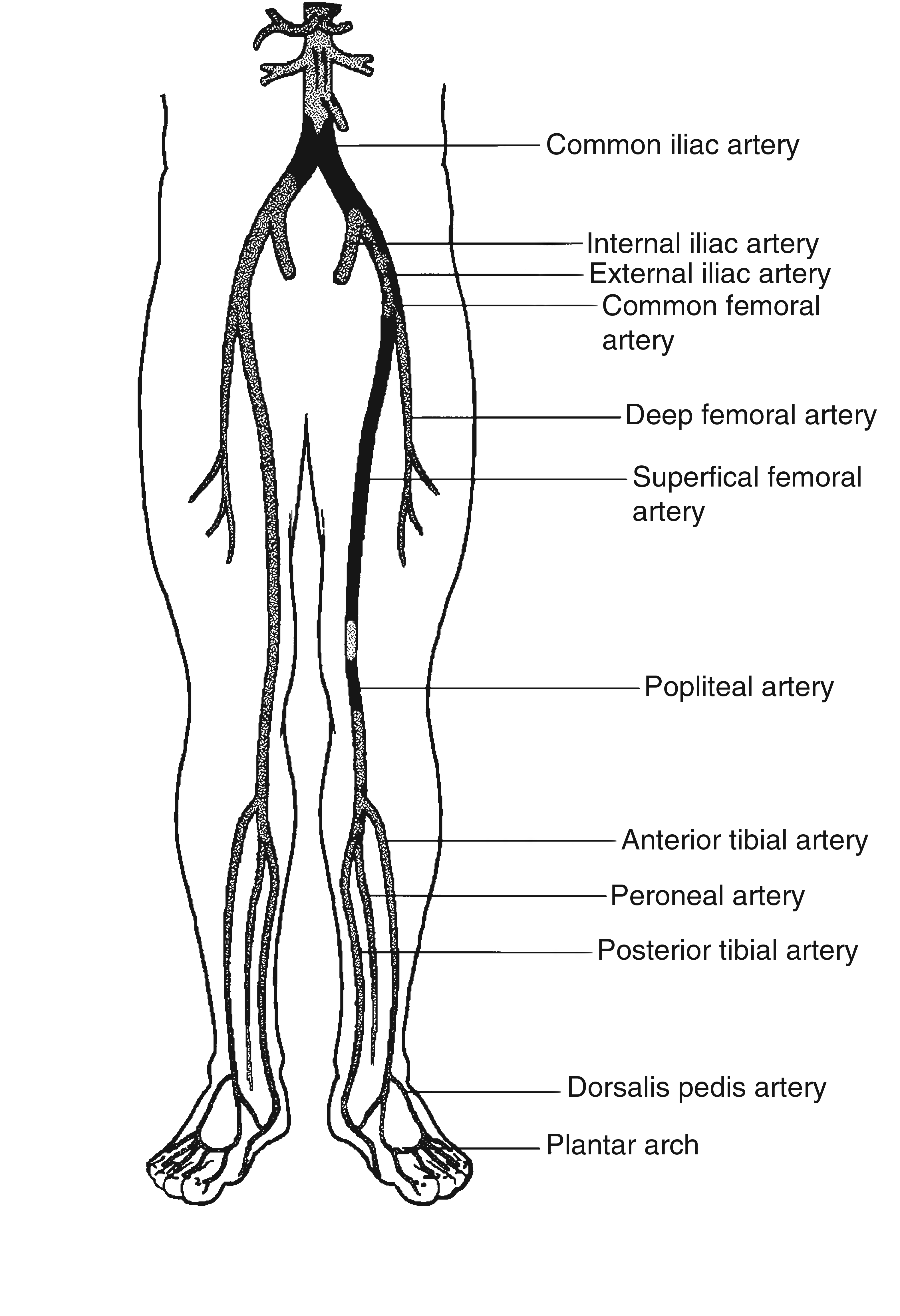
At its most distal aspect, the aorta branches to form paired common iliac arteries.
These continue retroperitoneally to the pelvic brim, at which the common iliac vessels branch to form paired internal and external iliac arteries. The internal iliac (or hypogastric) arteries provide blood supply to the pelvic structures, while the external iliac courses inferior to the inguinal ligament to become the common femoral artery.
The common femoral artery then bifurcates early in its course to form the profunda femoris artery, which supplies the thigh musculature, and the superficial femoral artery, which continues inferiorly to become the popliteal artery at its point of entry into the adductor canal.
The popliteal artery then continues below the knee, where the anterior tibial artery branches, piercing the interosseous membrane to supply the anterior compartment of the lower leg. The tibioperoneal trunk then continues briefly, where the posterior tibial artery branches to course in a plane deep to the soleus muscle. The vessel then continues inferiorly as the peroneal (fibular) artery.
The posterior tibial artery is divided into lateral and medial plantar arteries below the medial malleolus to supply the sole of the foot. Ultimately, the anterior tibial artery continues on to the dorsum of the foot, where it becomes the dorsalis pedis artery. Here it anastomoses with branches of the posterior tibial and peroneal arteries to form the plantar arch. On the dorsum of the foot, the dorsalis pedis artery forms two branches: the dorsal metatarsal and the deep plantar arteries. The deep plantar artery penetrates into the sole of the foot and joins the lateral plantar artery (branch of the posterior tibial artery) to form the plantar arch.
Collateral Circulation
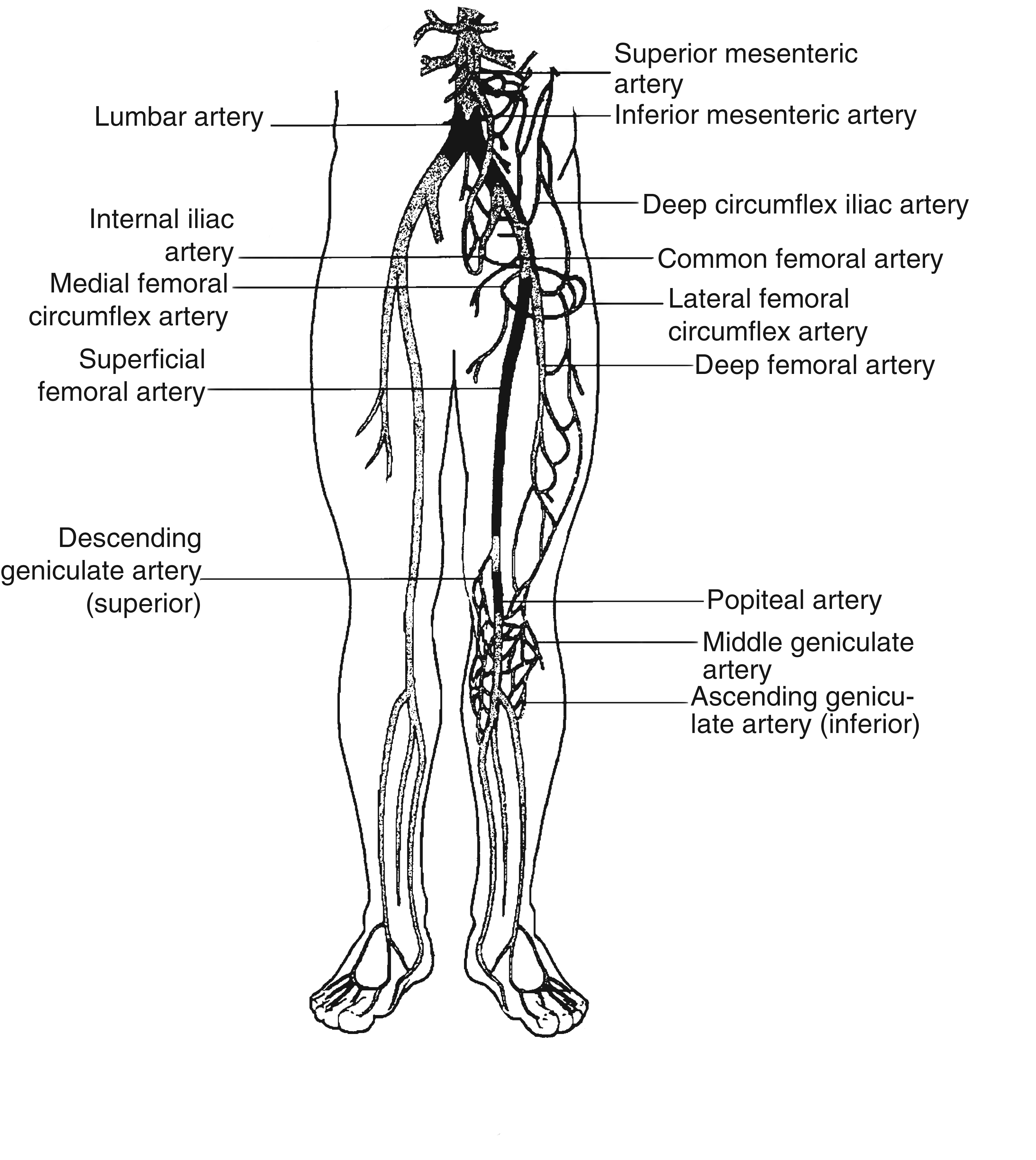
In the event of chronic obstruction of major arterial vessels, collateral pathways exist that allow preservation of sufficient distal blood flow to maintain viability of the tissues distally. The degree of adequacy of these pathways determines what degree of functional disability results. With obstruction at the level of the distal aorta and common iliac arteries, a variety of pathways for collateral circulation exist. Communications may exist between the lumbar and circumflex iliac or hypogastric arteries. Other communications may exist between the gluteal branches of the hypogastric arteries and recurrent branches of the common femoral or profunda femoris arteries. Visceral–parietal communications may also exist at this level between the inferior mesenteric