Behavioural Sleep Medicine, 12:1-12, 2014
DOI: 10.1080/15402002.2013.82906
Anna Kisa,b, Sára Szakadáta,c, Klára Horváthd, Péter Simora,e, Ferenc Gombosc,f & Róbert Bódizsc,e
NOTE: Anna Kis and Sára Szakadát contributed equally to this work.
a Department of Cognitive Sciences , Budapest University of Technology and Economics
b Research Center for Natural Sciences, Institute of Cognitive Neuroscience and Psychology, Hungarian Academy of Sciences, Budapest , Hungary
c Institute of Behavioral Sciences, Semmelweis University, Budapest , Hungary
d Department of Cognitive Science, Budapest University of Technology
e Department of General Psychology, Pázmány Péter Catholic University , Budapest , Hungary
f Department of Experimental Psychology , University of Oxford
Correspondence should be addressed to Róbert Bódizs, Institute of Behavioral Sciences, Semmelweis University, Budapest, Hungary, H-1089, Nagyvárad tér 4. E-mail: bodrob@net.sote.hu
Abstract
The first-night effect—marked differences between the first- and the second-night sleep spent in a laboratory—is a widely known phenomenon that accounts for the common practice of excluding the first-night sleep from any polysomnographic analysis. The extent to which the first-night effect is present in a participant, as well as its duration (1 or more nights), might have diagnostic value and should account for different protocols used for distinct patient groups. This study investigated the first-night effect on nightmare sufferers (NM; N D 12) and healthy controls .N D 15/ using both objective (2-night-long polysomnography) and subjective (Groningen Sleep Quality Scale for the 2 nights spent in the laboratory and 1 regular night spent at home) methods. Differences were found in both the objective (sleep efficiency, wakefulness after sleep onset, sleep latency, Stage-1 duration, Stage-2 duration, slow-wave sleep duration, and REM duration) and subjective (self-rating) variables between the 2 nights and the 2 groups, with a more pronounced first-night effect in the case of the NM group. Furthermore, subjective sleep quality was strongly related to polysomnographic variables and did not differ among 1 regular night spent at home and the second night spent in the laboratory. The importance of these results is discussed from a diagnostic point of view.
Introduction
A phenomenon that all polysomnographic sleep studies—basic or clinical—encounter is the first-night effect—a marked difference between sleep quality of the first and second night spent in the sleep laboratory. Distinct patient groups—in addition to their altered sleep patterns—can also show first-night effect to a different extent. Based on this argument and due to the lack of data available on the first-night effect in different clinical populations, this study aims to investigate this effect by combining objective and subjective methods in nightmare sufferers (NM) and healthy controls (CO). The first-night effect refers to a set of differences observed on the first recording, compared to consecutive ones—most commonly, the second one (Agnew, Webb, & Williams, 1966). Specifically, compared to the recordings of the second night, first-night sleep is characterized by decreased total sleep time and reduced REM sleep, lower sleep efficiency, more intermittent wake time, longer REM latency, and an increased amount of Stage-1 (S1) sleep (Curcio, Ferrara, Piergianni, Fratello, & De Gennaro, 2004). The origins of this effect can be attributed to multiple reasons: unfamiliar environment, discomfort, limitations of movements because of the electrodes and cables, and the psychological consequences of “being under investigation” (Bon et al., 2003; Tamaki, Nittono, Hayashi, & Hori, 2005). As the first-night effect is a direct consequence of the objective—polysomnographic—sleep assessment along with the laboratory setting, it has scarcely been investigated by subjective measures, such as self-rating questionnaires, indexing sleep quality. Furthermore, the comparison of subjective reports and objective (polysomnographic) measurements of different sleep parameters, in general, has only been done in a very few studies. Whereas the first such study (Johns, 1975) found that objective and subjective measures were related, more recent studies found a marked discrepancy between the two measures (Philipsen et al., 2005)—for instance, regarding the length of sleep and the latency of sleep onset (e.g., Silva et al., 2007). Moreover, in a recent study (Moser, Kloesch, Fischmeister, Bauer, & Zeitlhofer, 2010) on healthy participants, the first-night effect was not detected by the examination of subjective sleep variables in contrast to the objective ones. Because of the observed differences between the first and the consecutive night spent in the sleep laboratory, it is common practice to exclude the first-night recording from any polysomnographic analysis (Mendels & Hawkins, 1967). Although most differences have been observed by comparing the first and the second night, it has also been shown that residual effects are present beyond the second night (Le Bon et al., 2001), and this can question the validity of the data recorded even on the second night. This issue might be addressed when investigating different psychiatric disorders because—although no such systematic analysis has been carried out—it has been suggested that each medical condition might influence the first-night effect in different ways (Newell, Mairesse, Verbanck, & Neu, 2012). This idea is supported by a few studies providing evidence that, for example, patients with sleep apnea disorders (Le Bon et al., 2000) and idiopathic NM individuals (Nielsen et al., 2010) manifest a stronger first-night effect. In contrast, patients suffering from depression (Toussaint et al., 1995), insomnia (Edinger et al., 1997; Edinger et al., 2001), or posttraumatic stress disorder (PTSD; Saletu et al., 1996) manifest a less-pronounced first-night effect. Given that the medical conditions may affect the magnitude of the first-night effect, stronger and longer first-night effects might also bias the observed differences in the characteristics of the second-night sleep as compared to the CO group. Nightmare disorder is a prevalent parasomnia characterized by vivid and highly unpleasant dream experiences that frequently end in abrupt awakenings (Spoormaker, Schredl, & van den Bout, 2006) usually—but not exclusively—from REM sleep with a clear recall of the disturbing mentation. Idiopathic nightmares are distinguished from posttraumatic nightmares (which are necessarily associated with PTSD) and sleep terrors (which typically arise from non-REM sleep with no clear recall of the dream). Although questionnaire-based studies have shown that nightmares are related to impaired sleep quality (Lancee, Spoormaker, & van den Bout, 2010; Li, Zhang, Li, & Wing, 2010; Schredl, 2003), and NM participants exhibit significantly worse values on sleep- and health-related indexes (Krakow, 2006), the sleep architecture of NM individuals has scarcely been investigated. After the first inconclusive results (Fisher, Bryne, Edwards, & Kahn, 1970; Germain, & Nielsen, 2003), a recent study (Simor, Horváth, Gombos, Takács, & Bódizs, 2012) found that NM participants are characterized by altered sleep architecture showing impaired sleep continuity and emotion-related increases in REM propensity reflected by reduced sleep efficiency, increased wakefulness, a reduced amount of slow-wave sleep (SWS), and an increased number of nocturnal awakenings, especially from Stage-2 (S2) sleep. The main goal of this study was to investigate the first-night effect in NM and CO participants by combining objective and subjective methods. Our aim was to compare the macrostructural sleep parameters between the first and the second night spent in the laboratory in NM and CO groups; and, in addition, to reveal possible interactions between the two factors (Night Group). We were also interested to see whether a relation existed between the two types of data (objective and subjective) regarding sleep quality. Furthermore, to determine whether the firstnight effect is still present during the second night spent in the sleep laboratory, we compared subjective ratings of sleep quality after the laboratory nights with that of 1 night spent at home.
Methods
Participants
Participants were selected from a pool of approximately 1,700 university students who had completed online questionnaires assessing dream quality, including the Dream Quality Questionnaire (Bódizs, Simor, Csóka, Bérdi, & Kopp, 2008), the Hungarian version of the Van Dream Anxiety Scale (Simor, Kovács et al., 2009), and a 7-point Likert scale (0 D almost never, 1 D once or twice per year, 2 D every 2–3 months, 3 D once per month, 4 D twice per month, 5 D once per week, and 6 D more than once per week) with two items: one assessing the frequency of nightmares with awakenings and the other assessing the frequency of bad dreams without awakenings. Inclusion criteria for the NM group were determined on the basis of the International Classification of Sleep Disorders–Second Edition (American Academy of Sleep Medicine, 2005) criteria and Levin and Nielsen’s (2007) model of disturbed dreaming, including disturbed dreamers without abrupt awakenings. Participants reporting one or more nightmares or bad dreams per week in the retrospective questionnaires were assigned to the NM group, whereas individuals were assigned to the CO group only if they had less than two nightmares and bad dreams during the last year. NM participants were thoroughly interviewed about the frequency and content of their negative dream experiences. Those participants who reported the onset of negative dream experiences in relation to a traumatic event or indicated that the content of their dreams was somehow related to a prior trauma (such as physical attack, accident, sudden death of a close relative, etc.) were excluded from the study. Forty-two participants, 19 NM (10 men and 9 women; mean age D 20.87 ˙ 1.57 years) and 23 CO (11 men and 12 women; 21.57 ˙ 1.47 years), participated in the 2-night-long polysomnography recording. Data of 15 participants (7 NM and 8 CO) were excluded from further analysis in this study due to technical problems (noisy recordings, increased impedance values, and problems with the reference electrode), especially at the first night. Therefore, finally, the polysomnographic data of 12 NM (5 men and 7 women; 21:83 ˙ 2:45 years) and 15 CO (7 men and 8 women; 22:00 ˙ 2:45 years) participants were analyzed. Participants that were included in the study did not differ in age from the ones that were excluded: NM, t.17/ D 0:454, p D :656; CO, t.21/ D 0:621, p D :542; on the State-Trait Anxiety Inventory-Trait anxiety questionnaire (STAI–T; Sipos, Sipos, & Spielberger, 1994): NM, t.17/ D 0:425, p D :676; CO, t.21/ D 0:425, p D :676; on the Hungarian version of the Beck Depression Inventory (BDI– H; Rózsa, Szádóczky, & Füredi, 2001): NM, t.17/ D 1:898, p D :091; CO, t.21/ D 0:097, p D :924; and Groningen Sleep Quality Scale (Simor, Köteles, Bódizs, & Bárdos, 2009) scores: NM, t.17/ D 0:092, p D :928; CO, t.21/ D 1:112, p D :280; or in sleep efficiency during the second night: NM, t.17/ D 0:891, p D :385; CO, t.19/ D 0:808, p D :429.
Procedure
Participants were not allowed to drink alcohol and take drugs (except contraceptives) on the day and the previous day of the examination. They were asked to avoid napping and consuming caffeine on the afternoon of the sleep recordings. Participants were asked to fill out questionnaires upon arrival to the laboratory. The Hungarian version of the 20-item STAI–T (Sipos et al., 1994) was used to assess general levels of anxiety, and the short form of the Hungarian version of the BDI–H (Rózsa et al., 2001) was used to measure the extent of waking depressive symptoms in our participants. Sleep was recorded in two consecutive nights by standard polysomnography, including electroencephalography (recording sites: Fp1, Fp2, F3, F4, Fz, F7, F8, C3, C4, Cz, P3, P4, Pz, T3, T4, T5, T6, O1, and O2), according to the 10–20 electrode placement system (Jasper, 1958), left and right electrooculography (EOG), bipolar chin, and leg electromyography (EMG); electrocardiography (ECG); as well as abdominal and thoracic respiratory movements. The monopolar EEG electrodes were referred to the mathematically linked mastoids (A1 and A2), whereas the other measurements (EOG, EMG, and ECG) were bipolar. Impedances for the EEG electrodes were kept below 8 kO. Signals were collected, pre-filtered (0.33–1,500 Hz, 40 dB/decade anti-aliasing hardware input filter), amplified, and digitized at a sampling rate of 4,096 Hz/channel by using the 32 channel EEG/polysystem (Brain-Quick BQ132, Micromed, Mogliano Veneto, Treviso, Italy). A further 40 dB/decade anti-aliasing digital filter was applied by digital signal processing which low pass filtered the data at 450 Hz. The digitized and filtered EEG was subsequently down-sampled at 1,024 Hz. The timing of lights off was between 11:00 p.m. and 1:00 a.m., as determined by participants’ usual sleep habits. Morning awakenings were scheduled after 9 hr of undisturbed sleep, except if participants spontaneously woke up earlier. In addition, participants had to fill out the Hungarian version of the Groningen Sleep Quality Scale (Simor, Köteles, et al., 2009) for both nights after awakening the following morning. A subgroup of the participants (10 NM and 18 CO; 19 of them with a polysomnography recording for both nights spent in the laboratory) also filled out the Groningen Sleep Quality Scale after 1 regular night spent at home. This questionnaire is a 15-item list of sleep complaints that gives a global score of sleep quality ranging from 0 to 14, with the maximum indicating poor sleep quality (Mejiman, de Vries-Griever, & de Vries, 1988). The research protocols were approved by the ethical committee of the Institute of Behavioral Sciences, Semmelweis University, Budapest. All participants gave informed consent and received monetary compensation (approximately e20 [$28] in Hungarian Forints for their participation in the sleep laboratory investigations.
Analysis
Wakefulness and sleep stages of the recordings were manually identified coding 20-sec epochs according to standardized criteria (Minaritzoglou, & Vagiakis, 2008; Rechtschaffen & Kales, 1968) by four experienced sleep researchers (first night: Anna Kis and Sára Szakadát; second night: Péter Simor and Klára Horváth) who were blind to the group membership of the participants. A generalized estimating equation was used to test the effect of night (first or second in the laboratory) and group (NM or CO) on the following variables: sleep efficiency (percentage), wake after sleep onset (WASO)—after first-night S1 sleep episode (min); sleep latency—first non-S1 episode sleep (minutes); relative S1 duration (percentage), relative S2 duration (percentage), relative Stage-3 C Stage-4 (SWS) duration (percentage), relative REM duration (percentage), and REM latency (minutes). The interaction between Night Group was examined to see if there was a differential first-night effect in the two groups. Subjective sleep quality was assessed by the Groningen Sleep Quality Scale. We again tested the effect of night (first or second in the laboratory and at home) and group (NM or CO) using generalized estimating equations. Furthermore, subjective sleep quality across the groups was correlated with the sleep variables (applying multinominal logistic regression). The effect of STAI–T and BDI–H scores on the first-night effect was assessed by using a general linear model, with the difference between the first and the second night in terms of the polysomnographic variables and subjective sleep quality as the dependent variables and STAI–T and BDI–H scores as the covariates in the model.
Results
Data from the polysomnographic recordings indicated that, in accordance with our hypothesis, sleep was poorer on the first night, showing a more pronounced first-night effect in the case of the NM group (see Table 1). In the case of some variables, such as sleep efficiency, the main effect of both factors (night and group) was significant (see Figure 1). In the case of other variables, such as the relative S2 duration, neither of the two factors influenced the variable; however, a significant interaction was found among them (see Figure 2). The results regarding subjective sleep quality were in accordance with polysomnographic findings (see Figure 3). There was a significant effect of nights spent in the laboratory or at home, 2 (1, N D 27/ D 19:296, p < :001; and group, 2 (1, N D 27/ D 6:059, p D :014. There was no interaction between the two factors, 2 (1, N D 27/ D 1:099, p D :577. Moreover, the subjective Groningen Sleep Quality Scale scores were associated with several objective sleep measures: sleep efficiency .2 D 21:401; p D :045/, sleep latency .2 D 29:064; p D :004/, S1 duration .2 D 28:481; p D :005/, S2 duration .2 D 31:075; p D :002/, SWS duration .2 D 28:671; p D :004/, REM duration .2 D 32:364; p D :001/, and REM latency .2 D 26:525; p D :009/. No correlation was found with WASO .2 D 15:246; p D :228/. Our data showed that NM patients scored higher than CO participants on both the STAI–T, t.25/ D 4:855; p < :001; and the BDI–H, t.25/ D 5:770; p < :001. However, a general linear model, with the difference between the first and the second night in terms of the polysomnographic variables and subjective sleep quality as dependent variables and STAI–T and BDI–H scores as covariates, revealed that the scores obtained on the STAI–T and BDI–H questionnaires did not affect the extent to which the first-night effect was present in the given participant (p > :05 for all tests).
Discussion
In line with previous research (e.g., Curcio et al., 2004), our study found decreased sleep duration, lower sleep efficiency, longer WASO and decreased REM duration at the first night compared to the second, which is in accordance with the well-known phenomenon of the firstnight effect (Agnew et al., 1966). We also found previously unreported differences in the ratio of S2 and SWS between the first and the second night. Specifically, all participants spent more time in SWS in the second night, and the NM group also spent relatively more time in S2 in the second, compared with the first, night. In line with an earlier study on NM participants
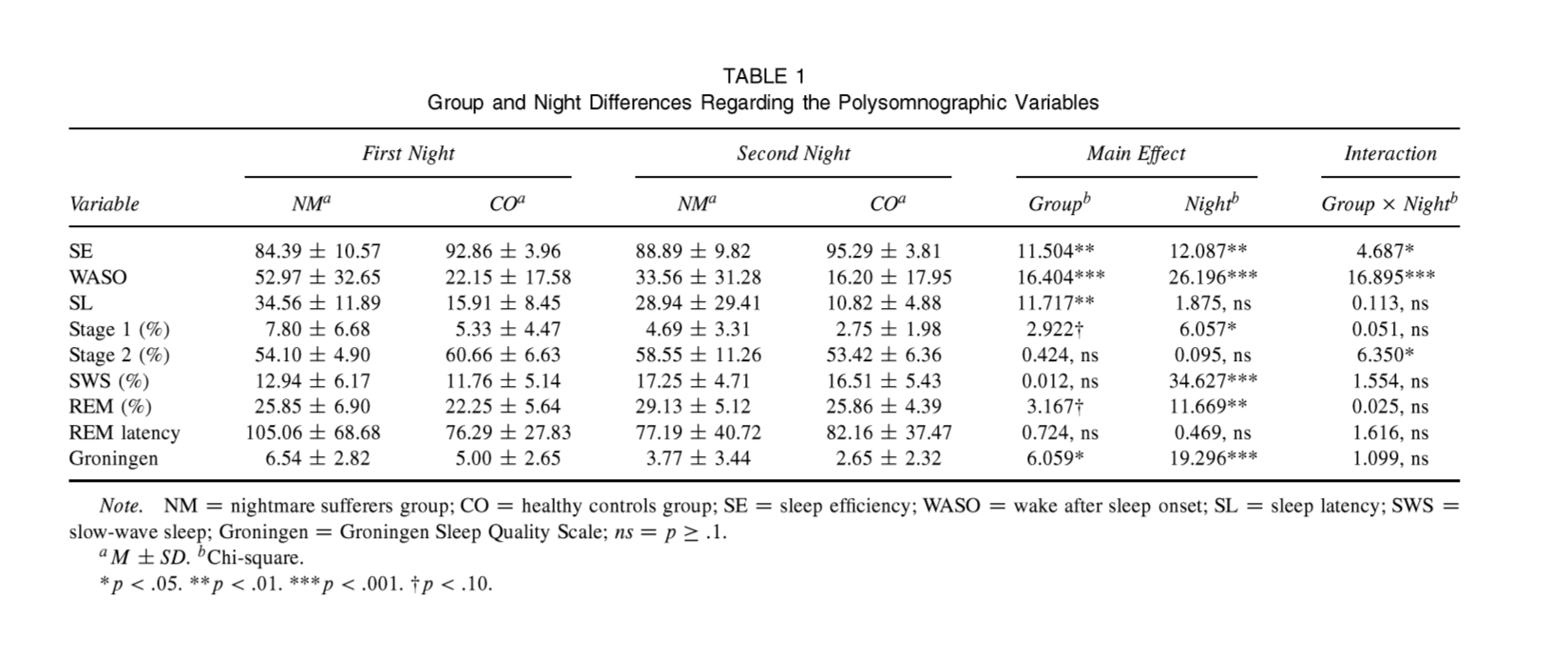
TABLE 1 Group and Night Differences Regarding the Polysomnographic Variables First Night Variable SE WASO SL Stage 1 (%) Stage 2 (%) SWS (%) REM (%) REM latency Groningen
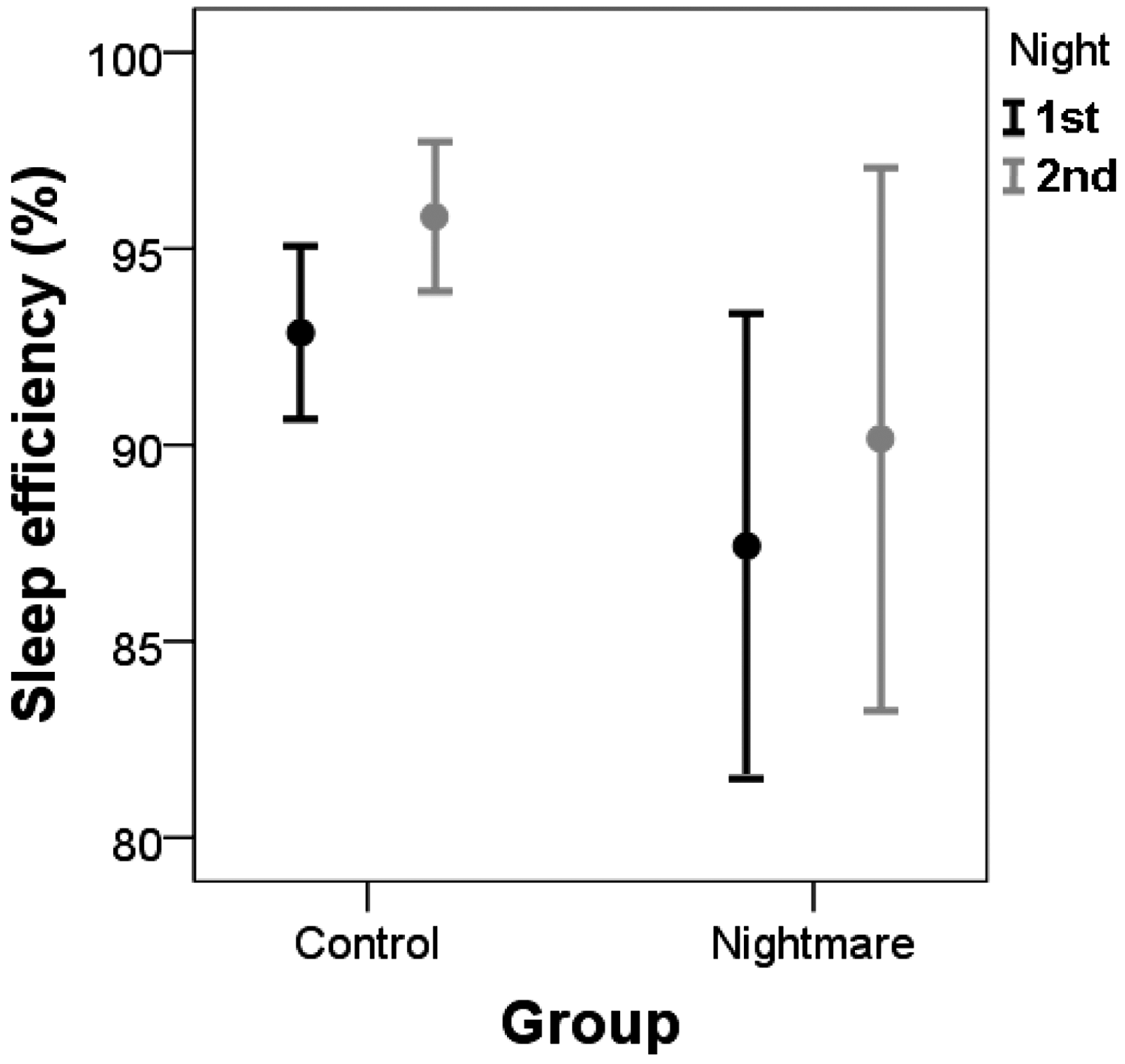
FIGURE 1 Sleep efficiency during the first and second night spent in the laboratory in nightmare sufferers and healthy controls (M+/-SD).
(Nielsen et al., 2010), our NM group was characterized by an enhanced first-night effect. Levin and Nielsen’s (2007) neurocognitive model explained this phenomenon by claiming that the discomfort and inconvenience of the sleep laboratory setting affect the NM group more due to their higher stress reactivity (Cernovsky, 1984; Coalson, 1995; Cook, Caplan, & Wolowitz, 1990; Hartmann, 1984; Picchioni et al., 2002). Our results are controversial in supporting this claim. Although the NM group scored higher than the CO group on anxiety and depression scales, these variables did not explain the magnitude of the first-night effect—neither
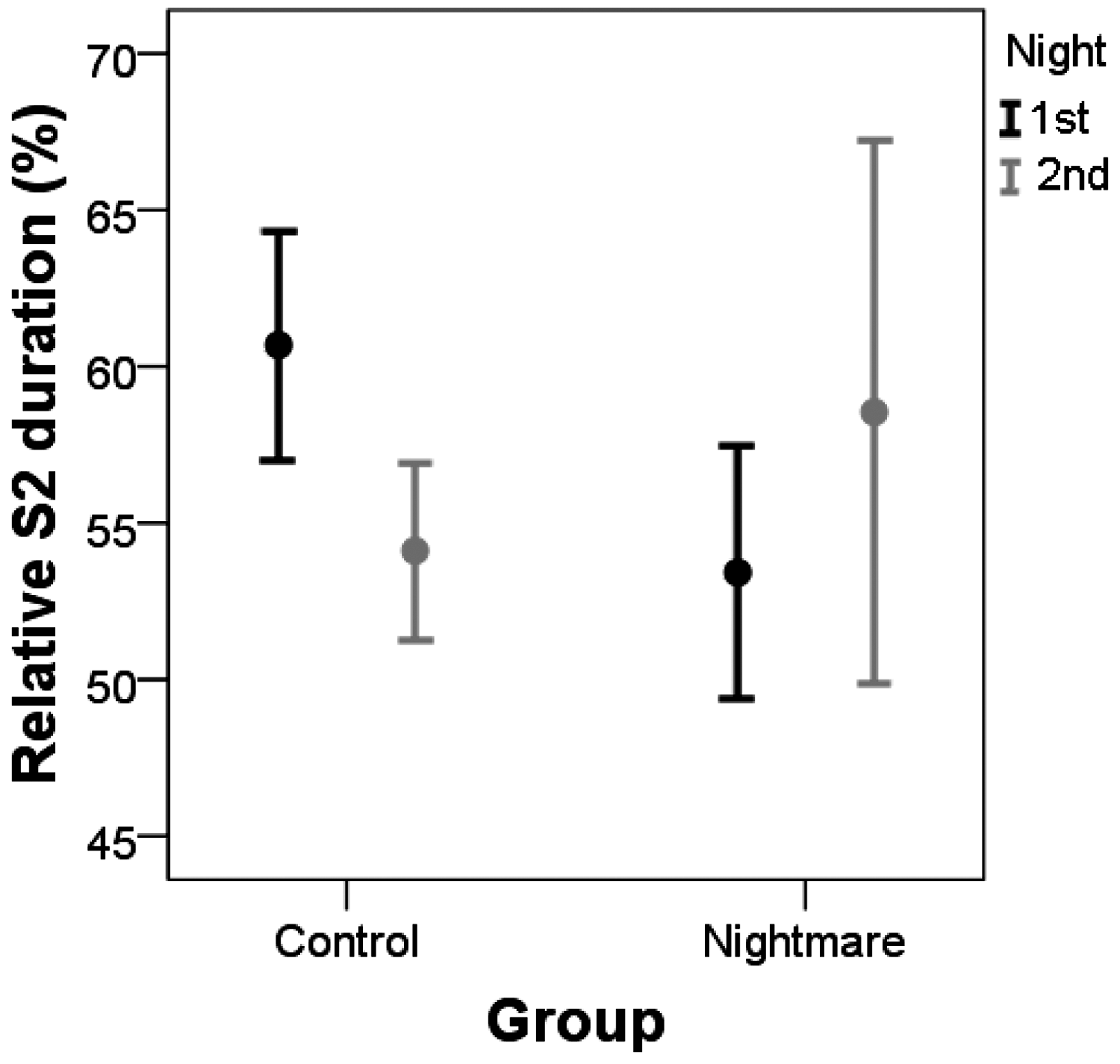
FIGURE 2 Relative Stage-2 duration during the first and second night spent in the laboratory in nightmare sufferers and healthy controls (M+/-SD).
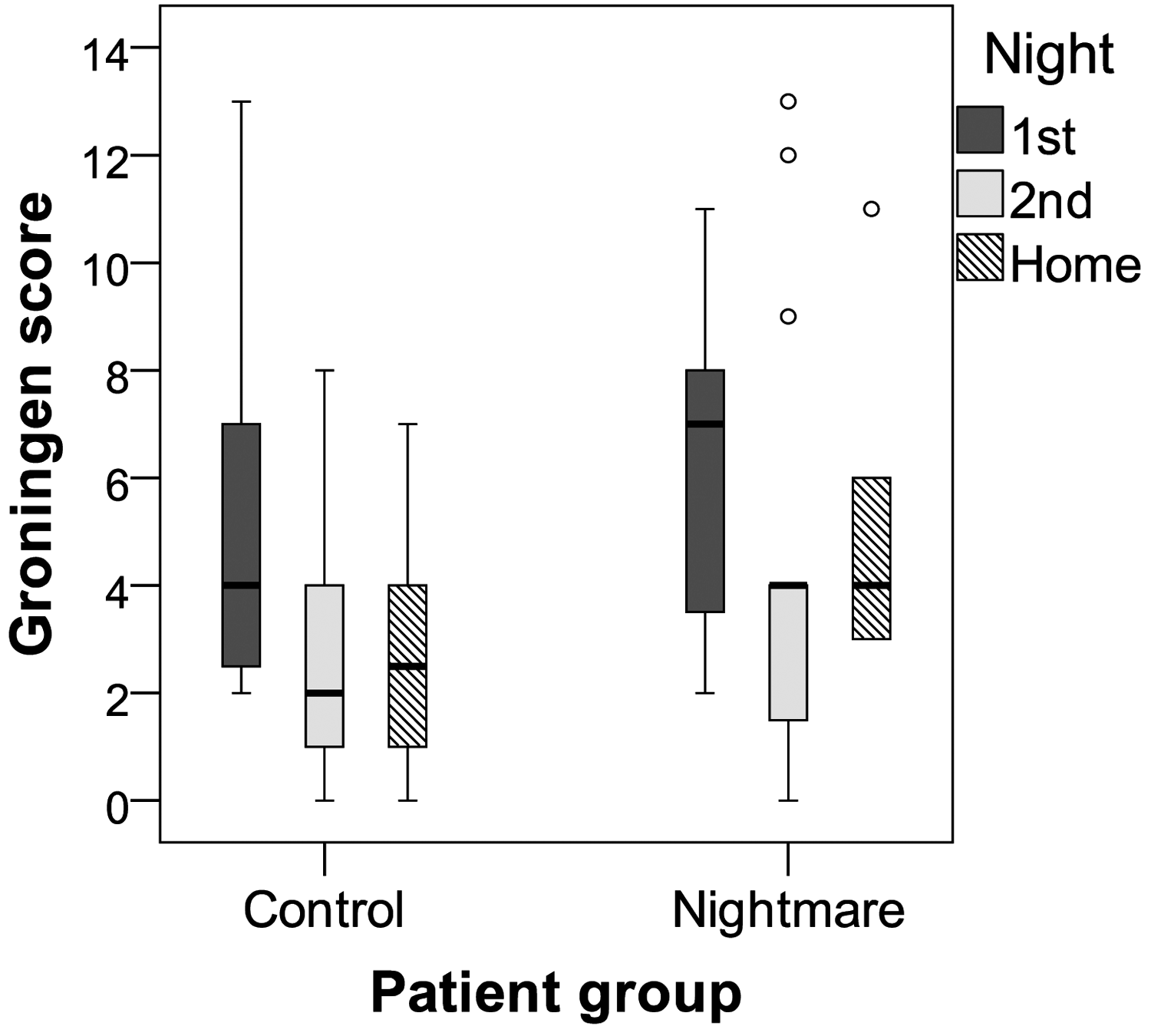
FIGURE 3 Box and whisker plots of Groningen Sleep Quality Scale scores of the two patient groups for the nights spent in the laboratory and at home. Note. Higher scores indicate impaired sleep quality. Horizontal bold lines D median; boxes D quartiles; minimum and maximum values D lower and upper whiskers; dots D outliers.
expressed by the objective, nor by the subjective measures. One potential explanation of this apparent inconsistency could emerge from the imprecise nature of psychometric instruments in characterizing the sleep laboratory-related discomfort and stress reactivity of our NM participants. Alternatively, these findings are in line with previous considerations (Spoormaker & Montgomery, 2008), suggesting that nightmare disorder should be conceptualized as a specific sleep disorder that is independent from comorbid psychopathological symptoms. It should also be noted that the difference between the first-night effect of the two groups mostly stems from a large baseline difference—namely, that the NM participants sleep much worse on the first night. Severely impaired sleep quality at the first night in the NM group, compared to that of the CO group, extends our previous results on a larger sample (Simor et al., 2012)—partly overlapping with this sample—showing disturbed sleep architecture in NM participants based on the recordings of the second night. Our study—in contrast to other results (e.g., Moser et al., 2010)—also revealed a difference in the participants’ subjective evaluations between the two consecutive nights, as reflected by the scores obtained on the Groningen Sleep Quality Scale. Moreover, this score was related to many objective sleep indexes in contrast to another study combining objective and subjective sleep measures, which found disagreement between the two (Silva et al., 2007). This might be attributed to the fact that, in this study, participants had to estimate specific parameters of their sleep—for instance, sleep latency or sleep length—so the “report biases” referred to the differences between the estimated and the exact values calculated from the polysomnographic data. There are no estimation requirements in the Groningen Sleep Quality Scale: We calculated an overall score about the subjective perception of the sleep quality based on yes–no answers given by the participants. This fundamental difference in the subjective method can explain the strong correlation we found between the data coming from the subjective and objective measures.
Along with the discussed theoretical contributions, our results may have practical consequences as well. It has been suggested earlier that the first-night effect might not be limited to the first night spent in the laboratory (Le Bon et al., 2001), which can question the validity of the data recorded on the second night. When investigating different medical populations, a pronounced first-night effect can cause the differences compared to the CO group. Our study did not find this pattern regarding idiopathic NM participants given that—similar to the CO group—the subjective score of the second night did not significantly differ from the score of the night spent at home. Participants with nightmare disorder even had a tendency to sleep better on the second night in the laboratory than at home, probably due to the partial sleep deprivation arising from the low sleep efficiency and reduced SWS observed during first night spent in the laboratory. Our results showed that the Groningen Sleep Quality Scale is a valid tool to assess participants’ baseline sleep quality (as measured at home). Thus, it might be used as an indicator of whether sleep in the laboratory differs from normal home sleep. Due to the lack of data available about the length of the first-night effect in specific medical conditions so far, the practical implementation of this questionnaire in all medical procedures is questionable, but it would contribute to the collection of valid—at least first-night effect free—objective sleep data. We should note, however, that due to technical problems—most commonly during the first night—we could only examine both nights’ recordings in a relatively small subset of our participants. Because the statistical power of our analyses is relatively low, our findings should be reproduced in subsequent experiments. Due to this small sample size, we could not exclude outliers from the analysis that might pose further limitations to our results. Moreover, the effects of the first night might influence sleep patterns on subsequent nights as well; therefore, investigations involving three or more laboratory nights would shed more light on the extended effects of the laboratory setting. Despite these limitations, our results draw attention to the fact that, in contrast to everyday practice—according to which the polysomnographic data recorded at the first night spent in the laboratory has to be excluded (Mendels & Hawkins, 1967)—the analysis of the first night’s sleep can provide valuable information. The differences between the sleep macrostructure of the first and second night are not necessarily the same in different medical conditions; therefore, future research about this phenomena might shed light on new diagnostic criteria.
Funding
This research was supported by the 2010 research grant of the BIAL Foundation (55/10). Anna Kis received funding from the Hungarian Scientific Research Fund (OTKA K100695). Péter Simor was supported by the European Union and the State of Hungary, co-financed by the European Social Fund in the framework of TÁMOP 4.2.4. A/1-11-1-2012-0001 “National Excellence Program.”
Acknowledgement
We acknowledge Réka Lihi, Adrián Pótári, Piroska Sándor, Zita Sulyok, and Réka Vida for their assistance in the polysomnographic recordings.
References
Agnew, H. W., Webb, W. B., & Williams, R. L. (1966). The first night effect: An EEG study of sleep. Psychophysiology, 2, 263–266. American Academy of Sleep Medicine. (2005). The International Classification of Sleep Disorders: Diagnostic and coding manual (2nd ed.). Westchester, IL: Author. Bódizs, R., Simor, P., Csóka, S., Bérdi, M., & Kopp, M. S. (2008). Dreaming and health promotion: A theoretical proposal and some epidemiological establishments. European Journal of Mental Health, 3, 35–62. Bon, O. L., Minner, P., Moorsel, V., Hoffmann, G., Gallego, S., Lambrecht, L., Linkowski, P. (2003). First-night effect in the chronic fatigue syndrome. Psychiatry Research, 120, 191–199. Cernovsky, Z. Z. (1984). Life stress measures and reported frequency of sleep disorders. Perceptual & Motor Skills, 58, 39–49. Coalson, B. (1995). Nightmare help: Treatment of trauma survivors with PTSD. Psychotherapy: Theory, Research, Practice, Training, 32, 381–388. Cook, C. L., Caplan, R. D., & Wolowitz, H. (1990). Nonwaking responses to waking stressors: Dreams and nightmares. Journal of Applied Social Psychology, 20, 199–226. Curcio, G., Ferrara, M., Piergianni, A., Fratello, F., & De Gennaro, L. (2004). Paradoxes of the first-night effect: A quantitative analysis of antero-posterior EEG topography. Clinical Neurophysiology, 115, 1178–1188. Edinger, J. D., Fins, A. I., Sullivan, R. J., Marsh, G. R., Dailey, D. S., Hope, T. V., Vasilas, D. (1997). Sleep in the laboratory and sleep at home: Comparisons of older insomniacs and normal sleepers. Sleep, 20, 1119–1126. Edinger, J. D., Glenn, D. M., Bastian, L. A., Marsch, G. R., Daile, D., Hope, T. V., Meeks, G. (2001). Sleep in the laboratory and sleep at home. II: Comparisons of middle-aged insomnia sufferers and normal sleepers. Sleep, 24, 761–770. Fisher, C., Byrne, J., Edwards, A., & Kahn, E. (1970). A psychophysiological study of nightmares. Journal of the American Psychoanalytical Association, 18, 747–782. Germain, A., & Nielsen, T. A. (2003). Sleep pathophysiology in posttraumatic stress disorder and idiopathic nightmare sufferers. Biological Psychology, 54, 1092–1098. Hartmann, E. (1984). The nightmare: The psychology and the biology of terrifying dreams. New York, NY: Basic Books. Jasper, H. H. (1958). Report of the committee on methods of clinical examination in electroencephalography. Electroencephalography and Clinical Neuroscience, 10, 370–375. Johns, M. W. (1975). Preliminary communication: Factor analysis of objective and subjective characteristics of a night’s sleep. Psychological Medicine, 5, 413–418. Krakow, B. (2006). Nightmare complaints in treatment-seeking patients in clinical sleep medicine settings: Diagnostic and treatment implications. Sleep, 29, 1313–1319. Lancee, J., Spoormaker, V. I., & van den Bout, J. (2010). Nightmare frequency is associated with subjective sleep quality but not with psychopathology. Sleep and Biological Rhythms, 8(3), 187–193. Le Bon, O., Hoffman, G., Murphy, G., De Meirleir, K., Cluydts, R., & Pelc, I. (2000). How significant are primary sleep disorders and sleepiness in the chronic fatigue syndrome? Sleep Research Online, 3(2), 43–48. Le Bon, O., Staner, L., Hoffmann, G., Dramaix, M., San Sebastian, I., Murphy, J. R., Linkowski, P. (2001). The first-night effect may last more than one night. Journal of Psychiatry Research, 35, 1656–1172. Levin, R., & Nielsen, T. A. (2007). Disturbed dreaming, posttraumatic stress disorder, and affect distress: A review and neurocognitive model. Psychological Bulletin, 133, 482–528. Li, S. X., Zhang, B., Li, A. M., & Wing, Y. K. (2010). Prevalence and correlates of frequent nightmares: A communitybased 2-phase study. Sleep, 33, 774–780. Mejiman, T. F., de Vries-Griever, A. H., & de Vries, G. (1988). The evaluation of the Groningen Sleep Quality Scale. Groningen, the Netherlands: Heymans Bulletin (HB 88-13-E). Mendels, J. D. M., & Hawkins, D. R. (1967). Sleep laboratory adaptation in normal subjects and depressed patients (“first night effect”). Electroencephalography and Clinical Neurophysiology, 22, 556–558. Minaritzoglou, A., & Vagiakis, E. (2008). Polysomnography: Recent data on procedure and analysis. Pneumon, 4, 348–368. Moser, D., Kloesch, G., Fischmeister, F. P., Bauer, H., & Zeitlhofer, J. (2010). Cyclic alternating pattern and sleep quality in healthy subjects—Is there a first-night effect on different approaches of sleep quality? Biological Psychology, 83(1), 206–226. Newell, J., Mairesse, O., Verbanck, P., & Neu, D. (2012). Is a one-night stay in the lab really enough to conclude? First-night effect and night-to-night variability in polysomnographic recordings among different clinical population samples. Psychiatry Research, 200, 795–801. Nielsen, T. A., Paquette, T., Solomonova, E., Lara-Carrasco, J., Popova, A., & Levrier, K. (2010). REM sleep characteristics of nightmare sufferers before and after REM sleep deprivation. Sleep Medicine, 11, 172–179. Philipsen, A., Feige, B., Al-Shajlawi, A., Schmahl, C., Bohus, M., Richter, H., Riemann, D. (2005). Increased delta power and discrepancies in objective and subjective sleep measurements in borderline personality disorder. Journal of Psychiatric Research, 39, 489–498. Picchioni, D., Goeltzenleucher, B., Green, D. N., Convento, M. J., Crittenden, R., Hallgren, M., & Hicks, R. (2002). Nightmares as a coping mechanism for stress. Dreaming, 12, 155–169. Rechtschaffen, A., & Kales, A. (1968). A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. Los Angeles, CA: UCLA Brain Information Service. Rózsa, S., Szádóczky, E., & Füredi, J. (2001). A Beck Depresszió Kérdoív rövidített változatának jellemzoi a hazai mintán [The short version of Beck depression scale in a Hungarian sample]. Psychiatrica Hungarica, 16, 379–397. Saletu, B., Klösch, G., Gruber, G., Anderer, P., Udomratn, P., & Frey, R. (1996). First-night effects on generalized anxiety disorder (GAD)-based insomnia: Laboratory vs. home sleep recordings. Sleep, 19, 691–697. Schredl, M. (2003). Effects of state and trait factors on nightmare frequency. European Archives of Psychiatry and Clinical Neuroscience, 253, 241–247. Silva, G. E., Goodwin, J. L., Sherrill, D. L., Arnold, J. L., Bootzin, R. R., Smith, T., Quan, S. F. (2007). Relationship between reported and measured sleep times: The Sleep Heart Health Study (SHHS). Journal of Clinical Sleep Medicine, 3, 622–630. Simor, P., Horváth, K., Gombos, F., Takács, K. P., & Bódizs, R. (2012). Disturbed dreaming and sleep quality: Altered sleep architecture in subjects with frequent nightmares. European Archives of Psychiatry and Clinical Neuroscience, 262, 687–696. Simor, P., Köteles, F., Bódizs, R., & Bárdos, G. (2009). A szubjektív alvásminoség kérdoíves vizsgálata: A Groningen alvásminoség skála hazai validálása [A questionnaire-based study of subjective sleep quality: The psychometric evaluation of the Hungarian version of the Groningen Sleep Quality Scale]. Mentálhigiéné és Pszichoszomatika, 10, 249–261. Simor, P., Kovacs, I., Vargha, A., Csoka, S., Mangel, B., & Bódizs R. (2009). Nightmares, dream anxiety and psychopathology: The validation of the Hungarian version of the Van Anxiety Scale. Psychiatrica Hungarica, 24, 428–438. Sipos, K., Sipos, M., & Spielberger, C. (1994). A State-Trait Anxiety Inventory (STAI) magyar változata [A State-Trait Anxiety Inventory (STAI)]. In F. Mérei & F. Zakács (Eds.), Pszichodiagnosztikai Vademecum I/2. Budapest: Nemzeti Tankönyvkiadó (pp. 123–148). Sipos, K., Sipos, M., & Spielberger, C. (1994). A State-Trait Anxiety Inventory (STAI) magyar változata [The Hungarian version of the State-Trait Anxiety Inventory (STAI)]. In F. Mérei & F. Zakács (Eds.), Pszichodiagnosztikai Vademecum I/2 (pp. 123–148). Budapest, Hungary: Nemzeti Tankönyvkiadó. Spoormaker, V. I., & Montgomery, P. (2008). Disturbed sleep in post-traumatic stress disorder: Secondary symptom or core feature? Sleep Medicine Review, 12, 169–184. Spoormaker, V. I., Schredl, M., & van den Bout, J. (2006). Nightmares: From anxiety symptom to sleep disorder. Sleep Medicine Reviews, 10, 19–31. Tamaki, M., Nittono, H., Hayashi, M., & Hori, T. (2005). Examination of the first-night effect during the sleep-onset period. Sleep, 28, 195–202. Toussaint, M., Luthringer, R., Schaltenbrand, N., Carelly, I. G., Lainey, E., Jacqmin, A., Macher, J. P. (1995). First-night effect in normal subjects and psychiatric inpatients. Sleep, 18, 463–469.