|
Semmelweis University, Institute of Behavioural Sciences, Budapest, Hungary Correspondence to L. Harmat: e-mail: laszloharmat@yahoo.com Accepted for publication 20 December 2007 AbstractTitle. Music improves sleep quality in students. Keywords: alternative therapy, depression, insomnia, psychology, sleep, stress IntroductionSleep quality is a very important factor in quality of life. Sleep disorders may result in fatigue, tiredness, depression and problems in daytime functioning. Several studies have focused on the effects of music on sleep quality, and researchers have found, in a variety of study settings and populations, that music positively affects sleep. The purpose of this research was to confirm the positive effects of music on sleep quality that the earlier studies have shown and investigate the specific effects of music on sleep quality by controlling for the confounding effect of relaxation and positive expectations. Most earlier researchers did not take into consideration these factors that may influence participants’ sleep quality and there remains the question whether music per se influences sleep or whether sleep quality is also affected by participants’ expectations of the treatment. BackgroundA number of studies conducted in clinical settings have suggested that sedative music may have positive effects on sleep via muscle relaxation and distraction from thoughts (Mornhigweg & Voigner 1995, Zimmermann et al. 1996, Johnson 2003, Lai & Good 2004). Music can reduce sympathetic nervous system activity, decrease anxiety, blood pressure and heart and respiratory rates (Standley 1986, Good et al. 1999, Salamon et al. 2003). Eight studies have had a direct focus on the effects of music on sleep. Zimmermann et al. (1996) studied the effects of relaxing music on sleep and pain in 96 patients who had undergone coronary artery bypass graft surgery. Levin (1998) examined the effects of ‘Brain Music’ in the treatment of 58 patients suffering from insomnia. ‘Brain Music’ is basically the transformation of spontaneous bioelectrical activity into music. Gitangali (1998) examined a traditional Indian ragha, which is similar to lullabies. Two studies have been conducted with children (Field 1999, Tan 2004). In Field’s study, children in the experimental group listened to music at naptime, while in Tan’s study they also did so at bedtime. Three researchers have investigated the effects of music on sleep in older adults (Mornhigweg & Voigner 1995, Johnson 2003, Lai & Good 2004). All studies showed that music had a statistically significant sleep-promoting effect, except for that by Gitangali (1998) in which no evidence was found for the positive effect of music on sleep. These results indicated that music is a potential non- pharmacological intervention for the treatment of sleep disturbances such as insomnia. However, they were based on self-report measures and have further limitations. For example, in most studies a control group was not used, whilst in theirs (Fried 1990a,b, Lai & Good 2004) music was combined with relaxation therapy or some other interven- tion, making it difficult to draw conclusions about the effects of music per se. The studyAim The aim of the study was to investigate the effects of music on sleep quality in young participants with poor sleep. Design A randomized controlled trial was used with a three group, repeated measures design was carried out in 2006. Participants Ninety-four students, 73 women and 21 men (mean age = 22,6 years, SD =2,83, range: 19–28), with sleep com- plaints were recruited at a university in Hungary. Participants were randomized using a computerized randomization table and variable block randomization. Each block was randomly assigned to the groups and the three groups in each block received only one ‘treatment’: listening to music (Group 1; n = 35), listening to an audiobook (Group 2; n = 30) or no intervention (Group 3; n = 29). The inclusion criteria were: Experimental interventions Members of the music group were given a CD containing classical music and were asked to accept or refuse the music collection. No participant refused it. The music was a collection of relaxing classical music including some popular pieces from Baroque to Romantic (The Most Relaxing Classical, 2 CD, Edited by Virgin 1999). We did not offer a choice of the type of music to be listened to, but all the participants confirmed that they liked classical music. The music was the same for all participants. The music collection was introduced to the participants by the investigators before the study and they were to listen to it for 45 minutes every night at bedtime for 3 consecutive weeks. All participants in the music group listened to 3-minute excerpts. The members of the audiobook group were given a CD containing 11 hours of short stories by Hungarian writers such as Frigyes Karinthy, Gyula Krúdy, Géza Gárdonyi, Zsigmond Móricz and Mihály Babits. Similarly to those in the music group, they were asked to listen to the audiobook at bedtime for 45 minutes each night for 3 consecutive weeks. They had the option to listen to new stories each night but could also listen repeatedly to the stories they preferred. All these participants listened to the same audiobook collection. The music and audiobook participants were asked to listen to their CD before going to bed and to avoid physical activities during and after the music or audiobook session. They had no previous training in any relaxation technique. Members of the control group did not receive any intervention, but participated in the pre- and postintervention assessment and were encouraged not to use music or an audiobook at bedtime. Measures The PSQI (Buysee et al. 1989) is a commonly used question- naire that measures self-reported sleep habits and can be completed in a short time. It gives information about the participant’s perceived sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, daytime dys- functions and use of sleep medication. These seven compo- nents form a global score that ranges between 0 and 21; the score for each component ranges from 0 to 3. Buysee et al. (1989) reported that score of 5 (indicating poor sleep) yielded a diagnostic sensitivity of 89,6 % and a specificity of 86,5 % and that the scale had good internal consistency, with α =0,83. A global PSQI score >5 is indicative of severe sleep difficulties in at least two areas… In order to develop the PSQI-H, the original PSQI was translated from English into Hungarian and then back- translated into English by an independent translator. We compared the original and the backtranslated PSQI ver- sions and created a preliminary Hungarian version. The Cronbach α coefficient in our study was α =0,79, indicating good internal consistency. Validation of the Hungarian version of the questionnaire is in process. In the present study, both the global PSQI and the component subscale scores were analysed so that the effects of music on individual elements of sleep could be determined. In the intervention groups, the PSQI was administrated four times: once before the intervention and subsequently at the end of each week during the study period. In the control group, the PSQI was used only twice, before and after the study, to minimize interference with usual practice and to avoid introducing any positive or negative expectations about sleep in this group. Mood and depression scores were measured by means of the BDI (Beck et al. 1961). We used a shortened version that is a modified version of the original shortened BDI (Beck & Beck 1972). The shortened version of BDI consists of 9 items and has been shown to have an internal consistency of a =0,85 in a nationwide representative Hungarian sample (Rózsa et al. 2003). On the basis of comparison of BDI and the shortened version, a reliable transformation of the scores of the shortened questionnaire into the original score is possible. (Kopp 1985, Kopp & Skrabski 1990). The items of the shortened questionnaire assess the existence and intensity of the following depressive symptoms: social withdrawal, inability to make decisions, sleep problems, fatigue, exagger- ated anxiety over somatic complaints, inability to work, pessimism, lack of satisfaction, difficulties with feeling pleasure and self-blame (Kopp et al. 1995). The BDI and its shortened version are reliable methods to measure the severity of depression. They correlate strongly with other estimates of depressive symptoms by psychiatrists. According to Eaves and Rush (1984), the severity of depression can be evaluated as follows:
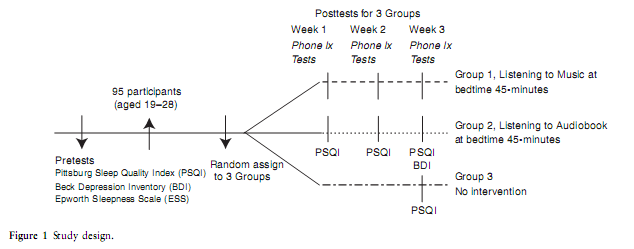
The ESS was used to assess depression and daytime somnolence. ESS is a simple, self-administrated questionnaire that measures general level of daytime sleepiness. Based on their recent way of life, participants rated on a scale from 0 to 3 the likelihood of dozing off or falling asleep in eight different situations commonly encountered in daily life. ESS values above 16 points are indicative of a high level of daytime sleepiness (Johns 1991). We used the ESS as a filter to exclude other sleep disturbances, such as obstructive sleep apnoea, periodic limb movement disorder, narcolepsy or idiopathic hypersomnia, which are associated with excessive daytime sleepiness. Data collection The study protocol is show in Figure 1. At the beginning of the study baseline data were collected using the PSQI, BDI and ESS and participants were randomly assigned to one of the three groups. During the following 3 weeks, the PSQI was completed weekly by participants in the music and audiobook groups. In the control group, we administered PSQI only on the third week. Participants in the music and audiobook groups also completed the BDI at the end of the intervention; in addition, we contacted the participants by telephone weekly during the study period to assess compliance with the protocol and all said that they complied.
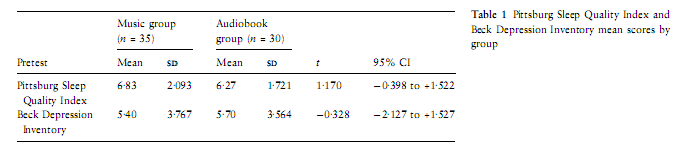
Ethical considerations The study was approved by the human research ethics committee of the study university. Participants received both oral and written information about the study signed an informed consent form. Data analysis We used parametric tests, i.e. paired samples t-tests, t-tests for independent samples and ANOVA with three groups. Independent sample t-tests were used to compare the PSQI and BDI scores of the two experimental groups at pretest and at weeks 1, 2 and 3. The Normality assumption was checked. A repeated measures ANOVA with main factors of GROUP (3 levels) and TIME (2 levels: pre and post) was used to analyse sleep quality between and within the three groups before and after the study. The assumptions of the parametric ANOVA model were also checked. Paired sample t-tests were used for within-group comparisons and Pear- son’s correlation was used to assess any linear relationship between PSQI and BDI scores in the experimental groups. The Bonferroni correction was used to control for Type I error with multiple testing, and the more conservative statistical significance threshold of 0,001 was set. Statistical analyses were performed using SPSS 12 and STATISTICA 7.0 ResultsPretest scores At pretest (first meeting) the global PSQI and BDI were c There were no statistically significant differences between the three groups in global PSQI scores.
PSQI and BDI outcomes in post-tests Global sleep quality and BDI scores
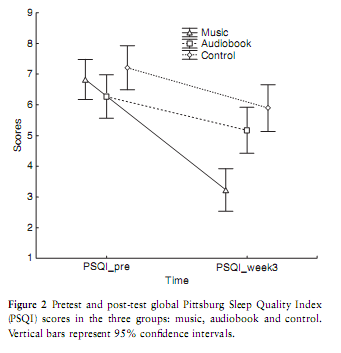
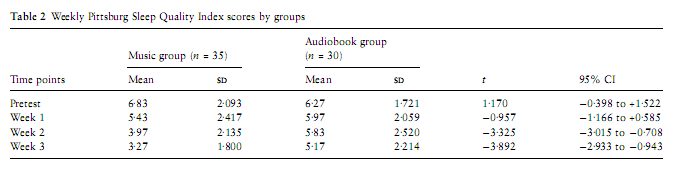
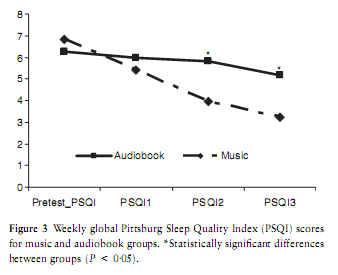
A repeated measures ANOVA with GROUP (3 levels) and TIME (2 levels) as main factors was used to analyse sleep quality within and between groups before and after the study. We did not find a statistically significant GROUP main effect. There was a significant main effect of TIME (F =87,157; P < 0,0001) and a significant interaction between TIME and GROUPS (F =14,748; P < 0,0001). Post hoc comparison (Bonferroni correction) of pretest scores with the three-weeks’ post-test scores showed that music significantly improved sleep quality (P < 0,0001).We did not find any improvement in sleep quality in the audio or control groups (Figure 2). We used t-tests for independent samples to compare weekly changes in global PSQI scores in the two intervention groups, i.e. music (Group 1) and audiobook (Group 2). We could not include the control group (Group 3) in these analyses as we had data on only two TIME points for this group. The magnitude of the difference between groups (music vs. audiobook) was statistically significant after the second week (week 2, P =0,0002 and week 3, P =0,0004). Improvement continued during the following week of the study (Table 2). Thus, listening to music has a cumulative effect on sleep quality (Figure 3).
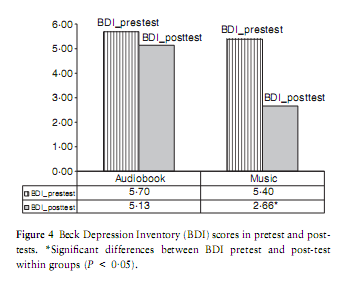
According to our results, music altered mood (Figure 4). Depressive symptoms decreased in the music group (t =6,124; P < 0,0001) but did not change statistically significantly after listening to audiobooks. The improvement of sleep quality (PSQI pretest minus PSQI3) correlated statistically significantly with decrease in depressive symptoms (BDI pretest minus BDI post-test) in the audiobook group (r =0,400; P =0,029), but this P value was not statistically significant when the Bonferroni correction factor was taken into account.
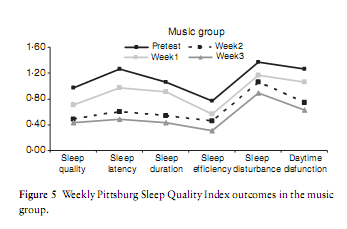
PSQI component scores The music group had statistically significantly better scores on the six PSQI components during the 3 weeks. A paired samples t-test was used to compare pretest scores and weeks 1, 2 and 3 scores within the music group. Listening to music resulted in improved subjective sleep quality, shorter sleep latency, longer sleep duration, better sleep efficiency, reduced sleep disturbances and less daytime dysfunction week by week; however, sleep duration showed a delayed effect since a statistically significantly longer sleep duration occurred during the second (t =4,098; P < 0,0001) and third weeks (t =4,828; P < 0,0001) in the PSQI tests (Figure 5). None of the PSQI components improved statistically significantly in the audiobook group. We measured PSQI components at the pretest and post-test assessment in the control group as well, but found no statistically significant changes in any of the component scores. Responders vs. non-responders Similarly to Lai’s study (Lai & Good 2004), we divided the participants into ‘responders’ and ‘non-responders’ after the intervention in the music and audiobook groups. Participants were considered responders if their total PSQI post-treatment scores dropped into the normal range (PSQI < 5). By the end of the study, 30 out of the 35 people (86%) in the music group responded to the intervention and became ‘good sleepers’, while five remained ‘poor sleepers’. In the audiobook group there were nine ‘responders’ (30%), while 21 from this group (70%) remained in the ‘poor sleepers’ range at the end of the study. There were differences in pretest scores between ‘responders’ and ‘non-responders’ from the music group. The pretest scores of the ‘responders’ were also statistically significantly lower on three of the six components of sleep quality: perceived sleep quality, sleep latency and sleep efficiency (P < 0,05). Lai and Good (2004) had the same results for pretest scores between ‘responders’ and ‘non-responders’. In our study, there were nine ‘responders’ in the audiobook group at the end of the intervention, while 21 participants remained in the ‘poor sleepers’ range. Among ‘responders’, we did not find statistically significantly lower pretest scores for any components of sleep quality. DiscussionThis is the first study to show that music per se improves sleep quality by controlling for the confounding effects of relaxation and positive expectations. Students who listened to sedative classical music for 45 minutes at bedtime for 3 weeks had better global sleep quality in the second and third week than those who did not. A possible explanation for the lack of a significant group main effect could be that the magnitude of difference between groups (music vs. audiobook) was statistically significant after the second week only. The improvement continued during the third week and more greater at the end of the study. The intervention was based on the effects of listening to music, but we do not yet have sufficient knowledge about the effects of music on sleep quality. Several studies conducted in clinical settings have suggested that sedative music may have positive effects on sleep via muscle relaxation and distraction from thoughts. Music can decrease sympathetic nervous system activity, as well as anxiety, heart rate, respiratory rate and blood pressure (Standley 1986, Good et al. 1999, Salamon et al. 2003). Several factors may help to explain our findings. One group of explanatory factors is related to the psychophysiological effect of musical tempo and the type of music that participants prefer. Reinhardt (1999) investigated the influ- ence of musical rhythm on the synchronisation and coordination of heart rate. Twenty-eight patients with chronic cancer pain in a stable phase of the disease underwent a 14- day relaxation training designed to improve the process of falling asleep. The therapy included 30-minute lullaby-like, rhythmically dominated music with gradually decreasing tempo. Reinhardt found that during the relaxation therapy trained patients showed increasing synchronisation and coordination of heart rate and musical beat. At a musical tempo between 48 and 42 beats/minute, a very stable 2:3 synchronisation was observed. Trained patients who reported the best relaxing and analgesic effects showed the highest degree of synchronisation. Bernardi et al. (2006) also confirmed that slow or meditative music can have a relaxing effect as well as an arousal effect, predominantly depending on the tempo. Sedative music with a slow tempo (42– 65 beats/minute) induces relaxation and reduces activity in the neuroendocrine system, and slow music produces a lower heart rate and blood pressure (Standley 1986). Salamon et al. (2003) confirmed that preferred classical music statistically significantly decreases systolic and diastolic blood pressure as well as anxiety levels. In addition, studies hav It is very important to differentiate between the efficacy of music in advancing sleep onset and its efficacy in improving sleep quality. In some studies (Fried 1990a,b, Lai & Good 2004) music was combined with relaxation therapy or with some other intervention, making it difficult to draw conclusions about the effects of music per se. In addition, a control group without any intervention has rarely been used, preventing investigation of the effects of the positive expectations of the experimental group. In contrast, we used a control group (no intervention) and an audiobook group to compare non-intervention and the effect of another intervention (listening to audiobooks) to listening to music. The auditory processes implied by listening to audiobooks are similar to those implied by listening to music. Elements of speech and musical sound can be characterized by the same parameters: pitch, duration, loudness, rhythmic metrical structure, contour, articulation and timbre. A large number of researchers have tried to reveal the similarities and differences between the two domains in the brain. A recent study has provided neurophysiological data to prove the similarity between listening to music and verbal material. In this research, Broca’s area, known for its specialization to syntactical processing in language, was also activated by music perception (Koelsch et al. 2002). This suggests that the mechanisms underlying syntactical processing are shared between music and language (Patel 2003). In addition, there is a similar brain response between speech and music boundary processing, and Kno ¨ sche also discovered EEG and EMG correlates for phrase boundaries in music. Neither music nor spoken language form uniform auditory streams; rather, they are structured into phrases (Kno ¨ sche et al. 2005). Despite the similar cognitive and neurobiological specificity of music and language, audiobooks had no effect on sleep quality in our study. The specificity of music may concern different processing components. Some processing components appear to be genuinely specialized for music (Peretz & Hyde 2003), while other components can be involved in the processing of both music and speech (Patel et al. 1998). Audiobooks also had no statistically significant effect on depressive symptoms in our study, as measured by the BDI. However, music decreased depressive symptoms scores in the experimental group. Several researchers have examined the therapeutic effect of music on depression (Hanser & Thompson 1994, Lai 1999, Hsu & Lai 2004) and found that music had beneficial effects on depressive symptoms. Music has been found to increase circulating endorphin levels (Mockel et al. 1994), which are associated with positive moods (Gerra et al. 1998). By the end of our study, mood scores had improved in the music group; however, our results suggest that music-induced improvement in sleep quality is not due to the effect of music on depressive symptoms. Nevertheless, this might be true in the case of audiobooks. The effect of music on sleep duration appeared later, since significantly longer sleep duration occurred in the second and third weeks in the PSQI tests. Sleep duration also showed a delayed improvement in a previous study (Lai & Good 2004). Listening to music in the present study resulted in reduction of global PSQI mean values to the normal range. Following the 3-week intervention, 30 out of the 35 members of the music group became ‘good sleepers’, while the global PSQI mean scores of the audiobook group remained in the ‘poor sleepers’ range. Study limitations The first limitation of our study is that participants were recruited as ‘poor sleepers’ (PSQI global score >5). They were healthy people with some sleeping problems which can return into the normal range without any intervention. Secondly, we used self-report measures of sleep without verifying them objectively. Thirdly, a 3-week study period may not be sufficiently long to draw any conclusions about the sustainability of improved sleep on longer time periods. Fourthly, the stories to which participants in the audiobook group listened to may have induced different emotions, while the emotional effect of slow classical music was considerably more balanced. Fifthly, we contacted by telephone every participant once a week to assess their compliance with the protocol, but we have no further information about how frequently they listened to music or to the audiobook during the study period. Finally, a Hawthorne effect may have occurred in the study. The Hawthorne effect refers to a phenomenon which is thought to occur when people observed during a research study temporarily change their behaviour and performance. Future research We recommend that researchers investigate the effects of music and audiobooks on sleep quality for more than three weeks. Music has a cumulative effect of sleep quality and our findings suggest that all poor sleepers might become good sleepers with a longer music intervention. It is also necessary to investigate the effects of music using objective, physiological measures of sleep such as polysomnography. Findings from the study by Lasic andOgilvie (2007), inwhich the effects ofmusic on sleep quality were investigated using a polisomnographic and quantitative EEG analysis, are not in line with our results. However, his study was conducted over a four-night period and such a short time is probably not sufficient to observe a positive effect of music on sleep quality. More research is needed to confirmthe effectiveness ofmusic on sleep quality in clinical populations such as in patients suffering from insomnia. However, it is difficult to find and enrol in a study patients suffering from insomnia who are medication-free. ConclusionOur findings provide evidence for the usefulness of relaxing classical music as an intervention for sleeping problems in young adults. In line with former studies, we confirmed that listening to relaxing classical music has a positive effect on sleep quality. Hospitalized patients often suffer from sleeping problems, such as insomnia, and listening to music is a simple intervention that may reduce these problems. Nurses should use music therapy in their practice because it is a safe and cheap method which may be used to treat insomnia in different populations. In addition, the intervention is quick and easy to learn.
AcknowledgementsThis work was supported by a PhD Grant from the Hungarian Ministry of Education, the National Office for Research and Technology (NKFP-1/B/020/04) and National Research Found (OTKA TS-049785). The authors were also supported by the Ferenc Faludi Academy (LH) and the János Bolyai Research Fellowship of the Hungarian Academy of Sciences (RB). Author contributionsLH, JT and RB were responsible for the study conception and design. LH and JT performed the data collection. LH and JT performed the data analysis. LH was responsible drafting of the manuscript. RB made critical revisions to the paper for important intellectual content. JT provided statistical expertise. LH and JT obtained funding. RB provided administrative, technical or material support. RB supervised the study. ReferencesBeck A.T. & Beck R.W. (1972) Shortened version of BDI. Post-graduate Medicine 52, 81–85. Beck A.T., Ward C.H., Mendelsohn M., Mosk J. & Erbaugh J. (1961) An inventory for measuring depression. Archives of General Psychiatry 4, 561–571. Bernardi L., Porta C. & Sleight P. (2006) Cardiovascular, cerebro- vascular, and respiratory changes induced by different types of music in musicians and non-musicians: the impotence of silence. Heart 92(4), 445–452. Buysee D.J., Reynolds C.F., Monk T.H., Berman S.R. & Kupfer D.J. (1989) The Pittsburg Sleep Quality Index: a new instruments for psychiatric practice and research. Psychiatry Research 28, 193– 213. Eaves G. & Rush A.J. (1984) Cognitive pattern in symptomatic and remitted unipolar major depression. Journal of Abnormal Psychology 93(1), 31–40. Field T. (1999) Music enhances sleep in preschool children. Early Child development and Care 150, 65–68. Fried R. (1990a) Integrating music in breathing training and relaxation: I. Background, rational, and relevant elements. Biofeedback and Self-Regulation 15, 161–169. Fried R. (1990b) Integrating music in breathing training and relaxation: II. Applications. Biofeedback and Self-Regulation 15, 171– 177. Gaston E.T. (1951) Dynamic music factors in mood changes. Music Educators Journal 37, 42–44. Gerra G., Zaimovic A., Franchini D., Palladino M., Guicastro G., Reali N., Maestri D., Caccavari R., Delsignore L. & Bambrilla F. (1998) Neuroendocrine responses of healthy volunteers to ‘technomusic’: relationships with personality traits and emotional state. International Journal of Psychophysiology 28(1), 99–111. Gitangali B. (1998) Effects of the Karnatic music raga ‘Neelembari’ on sleep architecture. Indian Journal of Physiology and Pharmacology 42, 119–122. Good M., Stanton-Hicks M., Grass J.M., Anderson G.C., Choi C.C., Schoolmester L. & Salman A. (1999) Relief of postoperative pain with jaw relaxation, music and their combination. Pain 81(1–2), 163–172. Hanser S.B. & Thompson L.W. (1994) Effect of a music therapy strategy on depressed older adults. Journal of Gerontology 49(6), 265–269. Hsu W.C. & Lai H.L. (2004) Effects of music on major depression in psychiatric patient.Archives of PsychiatricNursing 28(5), 193–199. Johns M.W. (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 14(6), 540–545. Johnson J.E. (2003) The use of music to promote sleep in older women. Journal of Community Health Nursing 20(1), 27–35. Knösche R.T., Neuhaus C., Haueisen J., Alter K., Burkhard Maess., Witte O.W. & Friederici A.D. (2005) Perception of phrase struc- ture in music. Human Brain Mapping 24, 259–273. Koelsch S., Gunter T.C., van Cramon D.Y., Zyset S., Lohmann G. & Friederici A.D. (2002) Bach speaks: a cortical ‘language-net- work’ serves the processing of music. NeuroImage 17, 956–966. Kopp M.S. (1985) Clinical psychophysiology, in Hungarian. Psychophysomatic Booklets 2, 1–35. Kopp M.S. & Skrabski Á. (1990) Methodology of comparative mental health studies, Article in Hungarian. Végeken 2(2), 4–24. KoppM.S., Skrabski Á. & Szedmák S. (1995) Socioeconomic factors, severity of depressive symptomatology and sickness absence rate in the Hungarian population. Journal of Psychosomatic Research 39(8), 1019–1029. Lai Y.M. (1999) Effects of music listening on depressed women in Taiwan. Issues in Mental Health Nursing 20(3), 229–246. Lai L.H. & Good M. (2004) Music improves sleep quality in older adults. Journal of Advanced Nursing 49(3), 234–244. Lasic S.E. & Ogilvie R.D. (2007) Lack of efficacy of music to improve sleep: polysomnographic and quantitave EEG analysis. International Journal of Psychophysiology 63(3), 232–239. Levin Ya. I. (1998) ‘Brain music’ in the treatment of patients with insomnia. Neuroscience and Behavioral Physiology 28(3), 330– 335. Mockel M., Rocker L., Stork T., Vollert J., Danne O., Eichstadt H., Muller R.& Hohrein H. (1994) Immediate physiological responses of healthy volunteers to different type of music: cardiovascular, hormonal, and mental changes. European Journal of Applied Physiology and Occupational Physiology 68(6), 451–459. Mornhigweg G.C. & Voigner R.R. (1995) Music for sleep distur- bance in the elderly. Journal of Holistic Nursing 13(3), 248–254. Patel A. (2003) Language, music, syntax and the brain. Nature Neuroscience 6, 468–488. Patel A.D., Peretz I., Tramo M. & Labrecque R. (1998) Processing prozodic and musical patterns: a neuropsychological investigation. Brain and Language 61, 123–144. Peretz I. & Hyde K. (2003) What is specific to music processing? Insight from congenital amusia. Trends in Cognitive Sciences 7, 362–367. Reinhardt U. (1999) Investigations into synchronisation of heart rate and musical rhythm in a relaxation therapy in patients with cancer pain, Article in German. Forsch Komplementar Medicine 6(3), 135–141. Rózsa S., Réthelyi J., Stauder A., Susánszky É .,Mészáros E., Skrabski Á. & Kopp M. (2003) A HUNGAROSTUDY 2002 országos reprezentatív felmérés általános módszertana és a felhasznált tesztbattéria pszichometriai jellemzői. Psychiatria Hungarica 18(2), 83– 94. Salamon E., Bernstein S.R., Kim S.A., KimM. & Stefano G.B. (2003) The effects of auditory perception and musical preference on anxiety in naive human subjects. Medicine Science Monitor 9(9), 396–399. Standley J.M. (1986) Music research in medical/dental treatment: meta-analysis and clinical application. Journal of Music Therapy 23(2), 56–122. Tan L.P. (2004) The effects of background music on quality of sleep in elementary school children. Journal of Music Therapy 41(2), 128–150. Zimmermann L.M., Nieveen J., Barnason S. & Schmaderer M. (1996) The effects of music intervention of postoperative pain and sleep in coronary artery bypass graft (CAGB) patients. Scholarly Inquiry for Nursing Practice 10(2), 153–170.
|