Digital intraoral scanner devices: a validation study based on common evaluation criteria
In addition to the confident use of intraoral scanning devices (IOS), knowledge of the desired intraoral scanner is indispensable for the precise fabrication of dental prostheses. New intraoral scanners are constantly emerging; however, comparing related studies can be challenging. In recent years, there has been a significant increase in research on intraoral scanners, but only some provide comprehensive evaluation of multiple devices based on the same criteria. There is a need for a unified protocol and standardized examination of intraoral scanners to provide all the information needed for practicing dentists.
We are pleased to announce that our study protocol was published in the international journal BMC Oral Health in 2022. The publication can be accessed via the following link: Róth I, Czigola A, Fehér D, et al. Digital intraoral scanner devices: a validation study based on common evaluation criteria. BMC Oral Health. 2022;22(1):140. Published 2022 Apr 26. doi:10.1186/s12903-022-02176-4 .
Approval for this study was given by the University Ethics Committee of Semmelweis University (SE RKEB number 108/2019).
The study on the comparative evaluation of intraoral scanners was renewed in September 2023, and accordingly, new types of documents were included in the study protocol. Therefore, for intraoral scanners tested after September 2023, more records are available on the respective pages compared to devices tested earlier.
This validation study aimed to compare intraoral scanners available in the Hungarian market based on objective and comprehensive parameters. The developed criteria are accessible on this page and are continuously updated with new intraoral scanners appearing on the market.
The intraoral scanners under examination are provided by the domestic distributors for the testing period. Both dentists experienced in digital impression taking and dental students participate in the study.
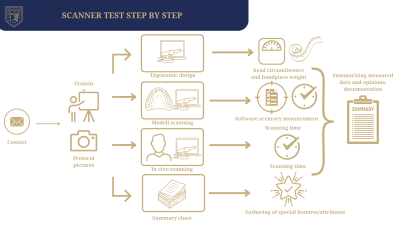
Step 1 of the study is training, which is provided in all cases by the distributors. The companies deliver training sessions similar to the ones they offer to the dentists interested in the scanners they distribute. The training consists of both theoretical and practical parts and lasts about one to two hours.
Step 2 of the study is the evaluation of the scanners. The evaluation of intraoral scanners consists of 5 points according to a validated set of criteria:
2/1. Short description
The documentation is compiled from the data provided by the manufacturer, international literature, and user experience during operation. It provides a comprehensive description of the scanner, mainly focusing on its technical properties (release date, contents, configurations, indications). The documents can be found on the website under the “Intraoral Scanners” tab.
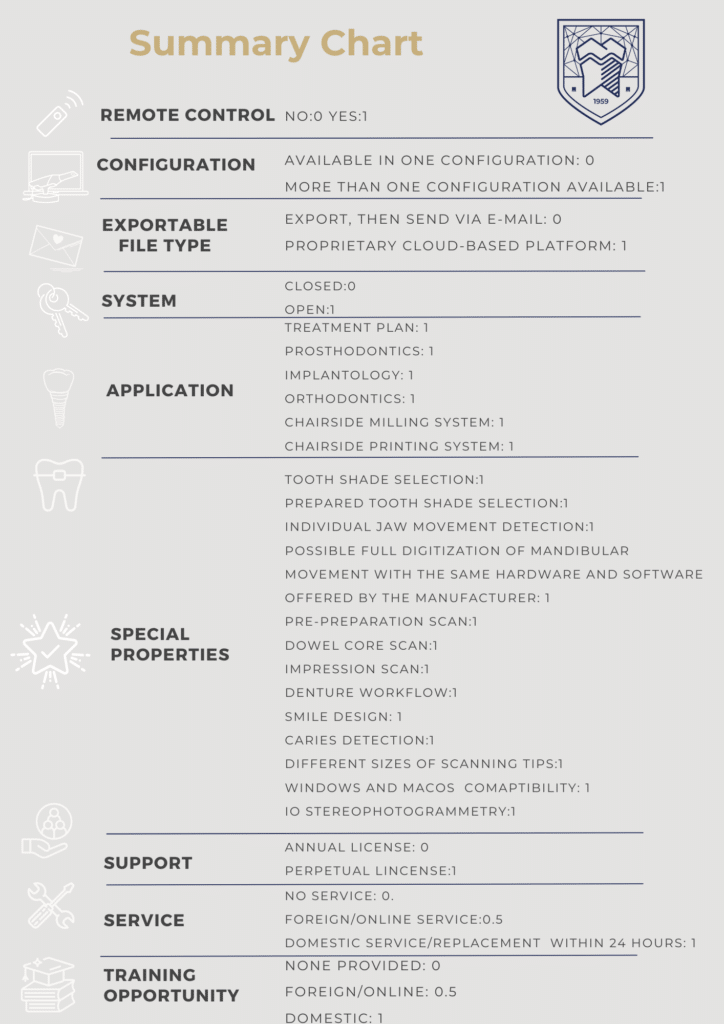
2/2. Summary Chart
The summary chart lists all important parameters that may influence users in choosing the appropriate intraoral scanner for their needs. The summary chart includes a total of 27 specific features that affect use, indication and evaluates which of these features characterizes the most the scanner in question. (Our previous protocol contained 21 specific features.)
2/3. Data recording sheet / Ergonomic parameters
This section provides information about the ergonomic design of the examined scanners. These details are not only important from the perspective of comfort, but scientific studies have confirmed that they also influence scanning accuracy. The diameter of the intraoral scanners head, and the weight of the scanners handpiece are measured.
2/4. Model scanning
Model scanning is performed for two purposes:
2/4.1. Accuracy (model scanning)
Based on the STL files generated during digital impression taking, accuracy measurements are carried out in the Geomagic Control X software package. During accuracy evaluation, the STL files created with the intraoral scanner are compared to the reference, which is the original model cast made from epoxy resin material and digitized with a high-precision laboratory scanner. The advantage of epoxy resin is that the sample does not need to be re-digitized before each examination with the reference scanner (3Shape E3 laboratory scanner), since epoxy resin materials possess excellent long-term dimensional stability.
2/4.2. Scanning time (model scanning)
The time required to scan a sample with prepared abutments during digital impression taking is recorded. (During impression taking, only the raw scanning time is recorded, i.e. without data acquisition or post-processing times.)
In our study, the previous in vitro protocol included scanning of one PMMA model (containing a single crown, an inlay cavity, and preparations for a bridge), which was scanned 10 times, each by 3 dental students. This simulated the situation when a dentist starts using a new intraoral scanner in their practice.
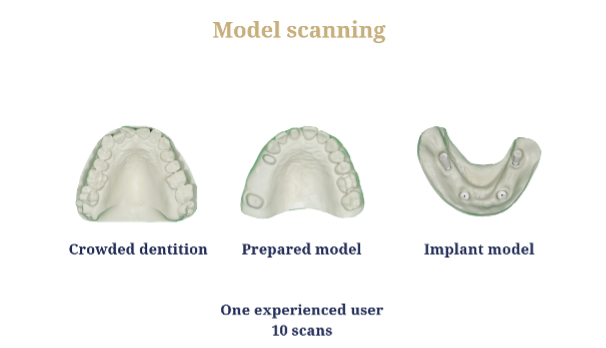
2/4.1. Accuracy (model scanning) – updated protocol
According to our new protocol in 2025, an experienced user scans 3 models, and their accuracy defines the indication range of the examined intraoral scanners:
- Crowded dentition model
- Model containing prepared teeth
- Edentulous mandibular model with Nobel CC implant analogs (all-on-x case with 4 implants in the mandible)
With each scanner, 1 experienced dentist performs all the scans and creates 10–10–10 digital impressions of the models. (Experienced = more than 3 years of experience in digital impression taking.)
Parameters measured for each model:
Crowded study model:
- WHL (Whole Deviation): Average deviation of the entire dental arch.
- Accuracy measurement performed on the segmented cut from the right to the left canine.
Prepared model:
- WHL (whole deviation), i.e. the average deviation of the entire dental arch.
- Prepared abutment of the upper right central incisor.
- Inlay cavity
- Distance between the upper right first premolar and second molar.
- Distance between the distobuccal cusps of the upper last molars represents a distortion of the entire dental arch.
Implant model (lower jaw, 4 Straumann implant analogs):
- WHL (whole deviation), i.e. the average deviation of the entire dental arch.
- Four distances were measured between implant analogs: 33-43, 36-46, 33-36, and 43-46 positions.
Accuracy results can be divided into two parts: those obtained according to the old protocol and those obtained according to the new protocol (from 2025). In the old protocol, accuracy results of 27 intraoral scanners are available, while in the new protocol, accuracy results of 9 intraoral scanners are currently available.
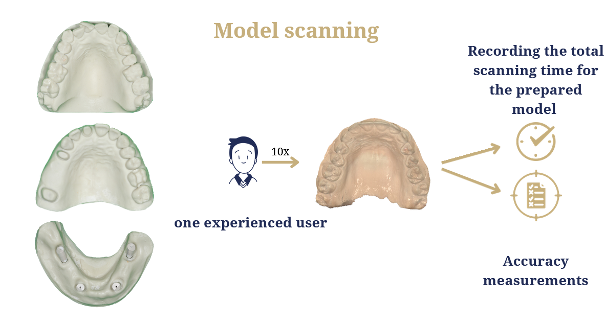
2/4.2. Scanning time (model scanning)
During digital impression taking, the time required to scan the prepared model is recorded. Only the raw scanning time is measured, meaning that data acquisition and post-processing times are not included.) The average time is calculated based on 10 scans.
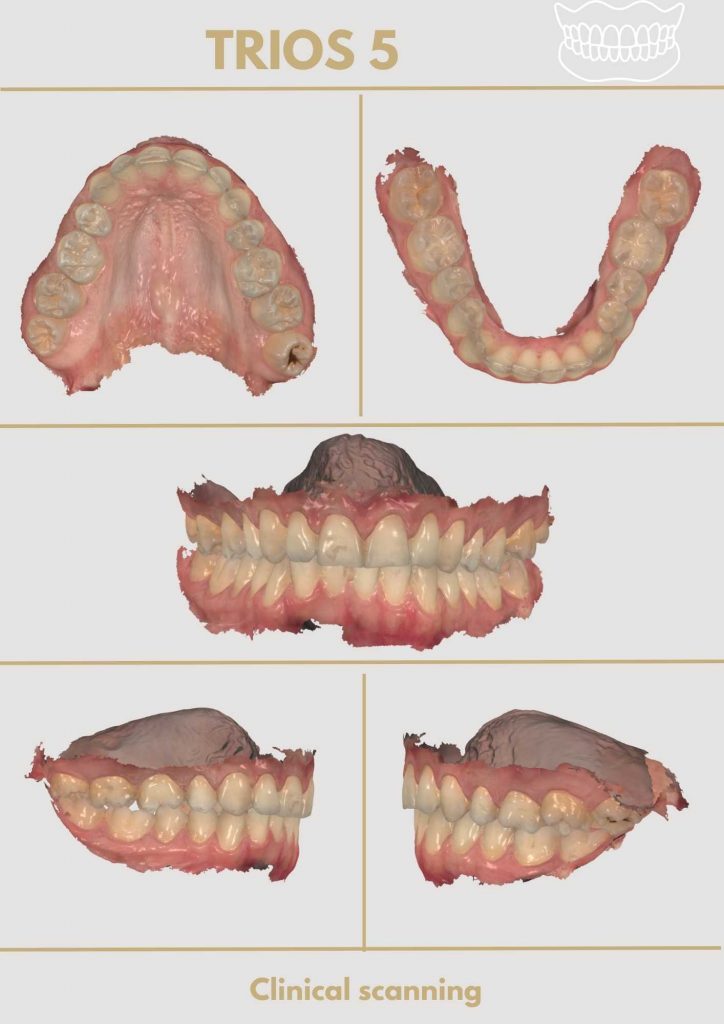
2/5. Clinical scanning:
In the course of clinical scanning, one experienced dentist scans a patient with a complete, preserved dentition three times (a total of 3 impressions). During the impressions, the complete upper and lower arches are scanned, and a bite registration is also performed in the intercuspidation position.
2/5.1. Scanning time (clinical scanning)
The raw time required for impression taking is recorded (data acquisition and post-processing times are excluded). The average time is calculated based on 3 impressions.
- No accuracy measurement is performed during clinical scanning.
Dental students scan a special articulated model on which both arches can be practiced, as well as the bite registration.
2/6. Step 3 of the study: Photographic documentation:
- Photographs of the scanner package contents, the scanner itself, and its various components
- Photographs of the scanner in use (in vivo) in its assembled state
- Screenshots of in vivo scans
- Screenshots of in vitro (model) scans
Step 4 of the study: Collection of subjective opinions (based on questionnaires).
The subjective questions are completed by all colleagues who participated in the training, assembled the scanner, scanned the articulated models including bite registration, and became familiar with the scanner’s software background. The subjective questions can be answered on a numerical scale from 0 to 10, and the last question requires a written response.
Questions:
- How would you rate the assemblability of the intraoral scanner?
- How ergonomic did you find the design of the scanner?
- How easy did you find the use of the software?
- During bite registration, how quickly and accurately was the software able to align the dental arches?
- During model scanning, how traceable was the finish line of the prepared teeth?
- How satisfied were you with the training provided by the distributor company?
- Would you be happy to use the examined scanner in everyday practice, or even later in your own dental office? Please justify your decision.
Summary chart
- Remote Control: The scanner can be controlled through hand gestures or voice commands without touching the screen, which is advantageous for infection control.
Available Score: whether the examined IOS had a remote control (1 point) or not (0 points).
- Configuration: The configuration of the intraoral scanner refers to how the hardware can be accessed. It may be available in single or multiple configurations (e.g., cart, MOVE, pod versions, and integrable versions into the control unit). Dentists can choose the most suitable configuration for their practice.
Available Score: 0 points were awarded if an IOS was available in a single configuration, and 1 point was awarded if there was more than one configuration.
- Open vs. Closed system: CAD/CAM systems can be categorized based on the method of data transmission: open and closed systems. Closed systems restrict file processing to the manufacturer’s CAD and CAM software, while open systems allow scanning data to be processed by various CAD/CAM systems.
Available Score: Open system: 1 point, closed system: 0 points.
- Application: In terms of indications, there are 5 types: intraoral scanners suitable for treatment planning, implantology, orthodontics or prosthodontics, and systems ideal for chairside use. Each of the 5 applications scores 1 point. The dentist performs scanning, designs, and mill restorations in a single session using a chairside system in the chairside workflow. The manufacturer provides CAD/CAM software and milling and sintering units for a fully equipped chairside system. It’s important to note that points are only awarded for chairside use if the company offers a complete package, including the intraoral scanner, chairside design software, milling machine/3D printer, and furnace. For implantology, points are awarded if the examined intraoral scanner is compatible with implantology software, enabling implant and abutment positioning design or surgical guide creation. Orthodontic usage includes access to orthodontic software for software-based orthodontic analysis, treatment planning, or designing orthodontic appliances.
- Special properties: All features enabling the intraoral scanner to perform more than just digital impression-taking are listed. Tooth and prepared tooth shade selection (the scanner is equipped with a built-in spectrophotometer capable of determining tooth shade simultaneously with digital impression taking), detection of individual jaw movements (capability for dynamic occlusal registration), pre-preparation scanning option (scanning old/temporary restorations or the patient’s teeth before tooth preparation within a single workflow), dowel core scanning, impression scanning, denture workflow, smile design (smile design with dedicated software), different-sized scanner heads, and caries detection. Each mentioned feature is worth 1 point.
- Support: Annual license renewal means the user must pay a certain amount annually to continue using the intraoral scanner and transmitting STL files. Failure to do so would render the scanner unusable. Alternatively, unlimited support means no need for a renewed license contract or costs proportional to the number of cases.
Available Score: Annual license renewal, costs proportional to the number of cases: 0 points, unlimited support through purchase: 1 point.
- Infrastructure: During clinical use, dentists can contact the distributor or manufacturer via email/phone/in-person for questions and receive prompt responses. Any hardware or software issues encountered during servicing are reported to the manufacturer/distributor for a solution. If the scanner has a Hungarian service, problems can be addressed quickly without shipping the scanner abroad. If the distributor provides a replacement device within 24 hours, which remains with the user until their scanner is repaired, it receives the maximum score akin to local servicing.
Available Score: Foreign/online service: 0.5 points, domestic service/replacement within 24 hours: 1 point (maximum 1 point can be scored).
- Training opportunity: Training can be provided by the scanner’s local distributor in a designated location and time in Hungary. This includes assembly, software usage, and scanning strategy demonstration. Training can also be conducted abroad, but this usually incurs higher costs for dentists and is typically conducted in English. Domestic or foreign courses may also be supplemented with online training materials.
Available Score: 0 points if no training is available from the distributor, 0.5 points for foreign or online coaching, and 1 point for domestic training.
Ergonomic Parameters
- Weight of the handpiece (g): The weight of the scanner headpiece is measured three times, and the average is calculated.
- Circumference of the scanner’s head (mm): The circumference of the scanner head is measured three times, and the average is calculated.
Model Scanning
- Scanning Speed (s): The clean scanning time is measured from the beginning to the end of the scanning process. This time is recorded, averaged, and evaluated. Data acquisition and post-processing times are not included in the scanning time.
- Accuracy: The STL files generated by the examined scanners are compared to the STL files created by the reference scanner for all 7 samples. The most important results are the study model results, as they are scanned by dental students every time. The overall deviation of the entire dental arch and crowded samples are reviewed for the study. The parameters for the prepared tooth sample are examined: average deviations on the whole sample, average deviations on the selected prepared tooth, and distance measurements (short/medium/long distance and total arch distance). The accuracy of the 26 cavity preparations is examined in the quadrant sample. The overall deviation of the entire dental arch and the average deviations of the implant analog positions are compared to the reference for the implant samples.
Clinical Scanning
- Scanning Speed (s): The “clean scanning time” is measured from the beginning to the end of the scanning process. This time is recorded, averaged, and evaluated. Data acquisition and post-processing time are not included in the scanning time.
A photo protocol is one of the crucial steps in examining intraoral scanners, during which the same set of images is captured for each examined device. We take photos of the unpacking process of the intraoral scanner components, and part of the protocol involves sharing screenshots of both model and clinical scanning virtual models.
